



{kind=link}
The week before last, I was fortunate to be invited to attend the Collaborative for Integrated Home Care Aid Innovation Symposium: a group of committed individuals and organizations that are passionate about improving healthcare through home care. The goal of the summit, organized by the SEIU union for healthcare workers and unions, was to apply the “Triple Aim” principles to home care. With the realization that our current systems cannot support the increase in chronic disease and the aging population, the group was looking for innovative solutions through people, process, and technology, that could provide preventative care and follow-up care in a community setting.
The State of Washington
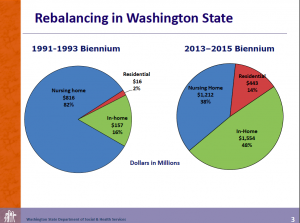
Bill Moss, Assistant Secretary for Aging and Long-Term Support, kicked off the day with a sobering look at the statistics for Washington State. While the number of people in nursing homes has declined by 7,000 since 1993, and more people are cared for in their homes, which provides a better quality of life, the complexity of health issues affecting the population has dramatically increased. In addition to being the preference of patients, at-home care is less expensive. If today we had as many people in long-term care facilities as 1993, it would cost the state an extra $200 M annually, so that’s good news.
Recognizing this benefit, but also understanding the increasing complexity of patients, provides a starting point for improving and supporting the role of home care workers to support more people aging at home. While return-on-investment studies are few and far between, the general understanding of participants is that keeping people out of long-term care facilities can provide financial subsidies to people in long-term care. For example, for the annual cost of one person in a nursing home, $17,500, three patients can be cared for in their homes.
To support these home care workers and their patients, new training needs to be developed to address some of the top health risks and preventative medicine including nutritional needs, fall risk, and mobility support. By helping people improve their health, we can save money and also improve quality of life.
Continuing on the data wallow, Lili Hay a researcher with Milliman, an independent consulting and actuarial firm, shared a deep dive into the situation in Washington and the complexity of patients that require home care, for example 40% of Medicare patients take 5 or more medications and most have more than one issue.
The Penn Center for Community Health Workers
Next up, Casey Chanton, a social worker and project manager at the Penn Center for Community Health Workers in Philadelphia talked about a unique program for training community leaders as health workers. In dealing with patients from low-income, high-health risk neighborhoods, physicians and patients had both expressed frustration with the gap between what physicians prescribed and the reality of patient’s lives. Physicians might tell a patient to eat a low sodium diet while the patient would be getting most of their meals from a food bank and have little or no control over what they ate. Both felt helpless to bridge the gap. Enter the community health worker. The program trained natural leaders from within these high-risk communities. These leaders visit patients in their homes and help them get the support they needed within the constraints of their own lives.
Not surprisingly, most of the issues were not medical but related to their living situations, income, and access to services. The best recruits to be community health workers were people who listened more than they talked and were non-judgmental. They helped patients set goals that were attainable by using patient-centered goal setting coupled with achievable steps.
Results of the program are impressive and really speak for themselves:
Panels on Technology Innovation and Practice Solutions
The next two sessions were panels, one on technology innovation and the second on practice options. There was too much good information for me to summarize everything, so I’ll stick to the major themes.
- Post-acute care costs are the fastest rising and most variable care costs, so finding a way to manage them is key.
- Technology is not the solution, people and process are the solution, but technology can help.
- People of all ages and socio-economic backgrounds can be use technology (although possibly not EMR interfaces—this isn’t a reflection on the people!)
- If we could start from scratch designing a health system, we would never have designed the siloed-system we have today.
- Issues of care coordination are causing post-acute care to be the fastest rising cost in healthcare today, even though readmissions are falling
- Homecare needs to be structured around outcomes not having homecare workers check off task lists
- Even if the payment models aren’t there yet, we need to take best practices and move forward.
- Even if all the research isn’t in, we need to take best practices and move forward.
- Even if healthcare administration isn’t ready for it, we need to take best practices and move forward.
During the panels and Q&A we heard from a few of the homecare workers in the audience about the impact they’ve had on people’s lives because they do what’s right and not what’s required. Particularly striking was the story from a woman who talked about caring for one of her patients who needed to go into a nursing home temporarily after surgery. The nursing home was understaffed so the homecare worker visited her patient there multiple times a day to make sure he was being turned in his bed. She did this because she cared about her patient and she wanted to make sure when he was released back into her care he wasn’t in worse condition than when he entered the nursing home. Rather than consider the negative aspects of this anecdote, let’s look at the amazing resource that exists in home care workers who spend more time with patients than their medical professionals and sometimes their families. That was the point of the day: what can we do to help scale this valuable resource and empower them to help patients even more.