



When national governments or global health funders have to decide whether to subsidize a new medical technology (a new vaccine, a new AIDS medication, a new clinical pathway), some ask whether the new technology is “cost-effective”, that is, whether the health gains from the introduction of the new technology outweigh the health given up or foregone as other activities are displaced to accommodate the additional costs.
When national governments or global health funders have to decide whether to subsidize a new medical technology (a new vaccine, a new AIDS medication, a new clinical pathway), some ask whether the new technology is “cost-effective”, that is, whether the health gains from the introduction of the new technology outweigh the health given up or foregone as other activities are displaced to accommodate the additional costs.
To answer this policy question, researchers often determine cost-effectiveness by comparing a new technology’s incremental cost-effectiveness ratio or ICER to a threshold that is some multiple of a country or income group’s GDP per capita, per WHO convention. The dollar value of the threshold is intended to represent the costs associated with health foregone or displaced by the adoption of the new technology.
In practice however, GDP-based thresholds have little empirical basis, as Shilcutt and co-authors lay out in their excellent review of decision rules and their use in studies related to low- and middle-income countries (LMIC). The lack of empirical justification for the decision rule can result in the adoption of unaffordable or inefficient technologies.
One example comes from middle-income countries considering the adoption of the Pneumococcal Conjugate Vaccine in various presentations (PCV-10 or PCV-13). Using the WHO’s CHOICE model and based on prices obtained via UNICEF, PCV in either presentation looks cost-effective when comparing the ICER of both kinds of PCV vaccine to a threshold of one to three times a GDP per capita. However, PCV will not likely be cost-saving at $16 a dose.
More Read


So the middle-incomes should adopt PCV, right? Unfortunately, the decision is not that clear: adding PCV at current prices could more than quadruple vaccination budgets if the entire birth cohort is targeted. In this case, assuming that the public budget will not grow to fully accommodate this new expenditure requirement** and that funds must be reallocated from other parts of the budget to this use, the GDP-based threshold is not reflecting the real opportunity cost of the allocation shift in the actual public budget that would be required to quadruple spending on immunization.
This is why work released last week by health economists at the University of York is so important: Karl Claxton and his co-authors have derived an empirically-based cost-effectiveness threshold for the UK’s National Health Service (NHS), which may be adopted by the priority-setting body NICE to issue guidance on new interventions.
While the actual value of the empirically-based NHS threshold is not relevant to LMIC, the methods and kinds of data used to estimate the threshold are highly relevant and could be used by LMIC and their external funders to guide future decision-making on new technology adoption.
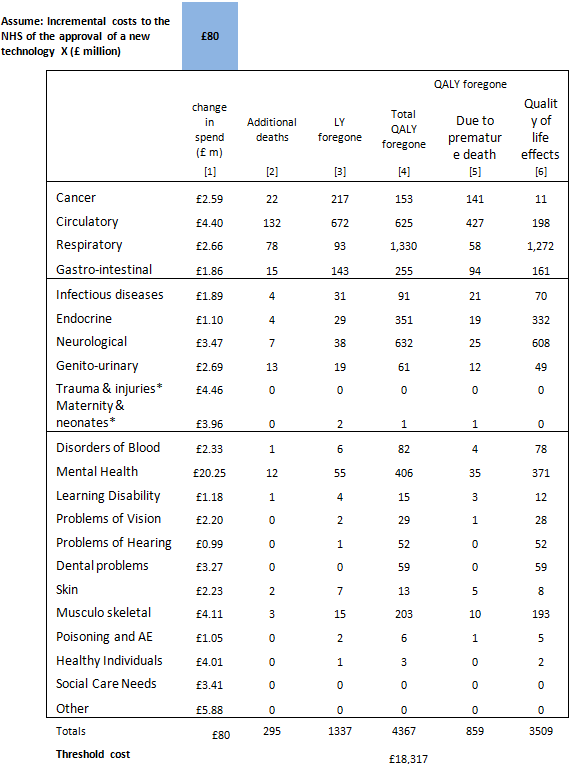
First, recognizing that the threshold would need to be revised periodically, the researchers started with the premise that they could only use data that was routinely available from the NHS. Second, they looked at the relationship between overall NHS expenditure and patients’ health outcomes. They write: “by exploiting differences between Primary Care Trusts [the commissioner or payer for health services in the NHS] in expenditure and outcomes, it is possible to infer the costs of generating health improvement from NHS services at the margin….[providing] an [average] indication of the health foregone through the services displaced by the additional budget effect” of any new technology adoption. The researchers also estimate a “budget elasticity of expenditure” within each program budgeting category* that allows for analysis of what will likely be cut –based on historical data- to accommodate the budget impact of a new technology. Finally, in addition to generating the new threshold, the team puts these two analyses together to come up with an app-like “health foregone calculator” table, shown below.
The table identifies: “how many QALYs are likely to be foregone across the NHS as a consequence of approving a technology which imposes incremental costs on the NHS (identified in blue cell). It can also indicate where those QALYs are likely to be foregone and how they are made up, i.e., the additional deaths, life years lost (unadjusted and adjusted for quality of life) and the quality of life impact on those with disease.”
The table shows that NICE’s recommendation of a new technology that had incremental costs of £80 million -such as Ranibizumab for the treatment of diabetic macular oedema- displaces the equivalent of 4,367 QALYs equating to 295 additional deaths and 1,337 life years foregone, most of which were likely to occur among patients suffering from cancer or circulatory, respiratory or gastro-intestinal disease.
This is the real opportunity cost that needs to be considered by policy-makers and the public in general.
No one expects cost-effectiveness to be the only criteria for decision-making on new technology adoption; indeed, our recent working group on priority-setting in health identified many other factors to consider and the importance of placing cost-effectiveness results within a fair and transparent process of decision-making.
But cost-effectiveness is among the most important criteria to consider since the health we give up may be as or more important than the health we gain from a new technology.
How much and what type of health lost by approving a new technology in the NHS?
Source: Claxton et al based on methods and results reported in http://www.york.ac.uk/che/research/teehta/methodological-research/#tab-4, Section 5.7.

*Each Primary Care Trust classifies its budget into “program budgeting categories” organized by disease-type, i.e., diabetes, respiratory care, etc.
**Of course, public budgets for health in middle-income countries are growing, and there is great diversity in the levels and growth rates of public spending within countries at the same or similar level of income. However, accommodating the higher incremental cost of new technologies is likely a challenge even in those countries where expenditure is growing rapidly.

{kind=link}