



Many public health policy experts believe that Medicare readmissions in the first 30 days after discharge are mostly avoidable and, therefore, indicative of poor quality care. As a result, Medicare has an initiative to reduce readmissions. However, health economist Austin Frakt points to several recent studies that raise doubts about the conventional wisdom. He opines:
Many public health policy experts believe that Medicare readmissions in the first 30 days after discharge are mostly avoidable and, therefore, indicative of poor quality care. As a result, Medicare has an initiative to reduce readmissions. However, health economist Austin Frakt points to several recent studies that raise doubts about the conventional wisdom. He opines:
[I]f we encourage hospitals to reduce readmission rates are we encouraging them to kill people?
The authors of the New England Journal of Medicine article explain:
More Read


Our findings suggest that readmissions could be “adversely” affected by a competing risk of death — a patient who dies during the index episode of care can never be readmitted. Hence, if a hospital has a lower mortality rate, then a greater proportion of its discharged patients are eligible for readmission.
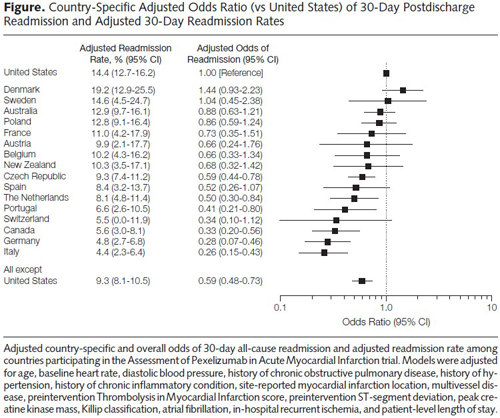
Another study finds the United States rates below almost all OECD countries in readmissions after a heart attack.


Countries with socialized health care systems tend to keep patients in the hospital longer because caring for a heart attack patient convalescing on Day 10 after an attack is far less costly than discharging the patient on Day 5 and admitting a new patient with a serious problem in their place. A convalescing “bed blocker” is a strategy hospitals use to avoid admitting more seriously-ill patients. In the United States, patients are typically discharged sooner to less-expensive facilities. For example, a patient might be discharged from a hospital and transferred to a skilled nursing facility; then later moved to a nursing home; and later discharged to home with home care nursing.
However, one must bear in mind that much of what drives hospital readmission rates are patient-and-community-level elements that are external to the hospital. More so, high readmission may not reflect poor quality, as Frakt is quick to point: high readmission rates can be the result of low mortality rates or good access to hospital care. Indeed, some studies show that improved external care coordination and access to follow-up care actually increases readmissions, hardly indicative of a failure of our health systems.




{kind=link}