




This occurred for many reasons, not the least of which was the reality that initiatives in healthcare ultimately comes down to driving patient and provider behavior. At the same time, the evolution of the various federal legislative actions were critical to driving this trend. There are obviously many health reward and incentive program legislative acts that have been proposed and/or passed, and we have outlined the history of some of the more noteworthy legislation here:
- 2004: Healthier Lifestyles and Prevention America Act (HeLP America). As noted above, on June 22, 2004, Senator Harkin proposed HeLP America, which included, among other things, provisions for the establishment of incentives for preventive health programs. Over multiple Congresses, Harkin introduced and championed HeLP America, which formed the basis of the Prevention and Public Health title of the Affordable Care Act (ACA) . The bill also included tax incentives for businesses that offer comprehensive workplace wellness programs to their employees, improved physical activity and athletic opportunities for individuals with disabilities, and greater oversight with regard to food and tobacco marketing. As Senator Harkin noted, “Some argue that avoiding obesity and preventable disease is strictly a matter of personal responsibility. Well, we all agree that individuals should act responsibly. I am all for personal responsibility. But I also believe in government responsibility. Government has a responsibility to make sure people have the information, tools and incentives to take care of their health. And that is what the HeLP America Act is all about.”
- 2005: Physician Quality Reporting System (Physician Quality Reporting or PQRS) formerly known as the Physician Quality Reporting Initiative (PQRI). PQRS is a reporting program that uses a combination of incentive payments and payment adjustments to promote reporting of quality information by eligible professionals (EPs). The program provides an incentive payment to practices with EPs. EPs satisfactorily report data on quality measures for covered Physician Fee Schedule (PFS) services furnished to Medicare Part B Fee-for-Service (FFS) beneficiaries. Beginning in 2015, the program also applies a payment adjustment to EPs who do not satisfactorily report data on quality measures for covered professional services. The PQRS program has roots in the quality improvement initiatives of 2005—and earlier movements to streamline and incentivize federally funded systems. In 2006, the Tax Relief and Health Care Act required the establishment of a quality measure reporting system for physicians to highlight evidence-based practice.The program was subsequently modified as a result of the SCHIP Extension Act. In the establishment stage since 2007, an incentive premium was available to all eligible professionals reporting, regardless of demonstrated improvement. However, since 2011, reporting 0% on any measure disqualifies participants from obtaining the incentive. In 2012, the program was changed from PQRI (Initiative) to the PQRS—Physician Quality Reporting System. The Affordable Care Act further expanded and deepened quality measure data reporting programs.
- 2006: Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the 2006 Wellness Regulations. Titles I and IV of HIPAA, Pub. L. 104-191, added section 9802 of the Code, section 702 of ERISA, and section 2702 of the PHS Act (HIPAA nondiscrimination and wellness provisions). These provisions generally prohibit group health plans and group health insurance issuers from discriminating against individual participants and beneficiaries in eligibility, benefits, or premiums based on a health factor. An exception to the general rule allowed premium discounts or rebates or modification to otherwise applicable cost sharing (including copayments, deductibles, or coinsurance) in return for adherence to certain programs of health promotion and disease prevention. Final regulations implementing the HIPAA nondiscrimination and wellness provisions were passed on December 13, 2006 at 71 FR 75014 (the “2006 Regulations”).The 2006 regulations divided wellness programs into two general categories: Participatory wellness programs and health-contingent wellness programs. Under the 2006 regulations, participatory wellness programs are considered to comply with the HIPAA nondiscrimination requirements without having to satisfy any additional standards if participation in the program is made available to all similarly situated individuals, regardless of health status. The 2006 regulations outlined five specific criteria that must be met for health-contingent wellness programs to comply with the nondiscrimination requirements, including that the total reward for wellness programs offered by a plan sponsor not exceed 20 percent of the total cost of coverage under the plan.
- 2008: Medicare Improvements for Patients and Providers Act of 2008 (“MIPPA”). MIPPA created a new incentive program for eligible professionals who are successful electronic prescribers (E-Prescribers) as defined by MIPPA. This program came to be known as the “E-Prescribing Incentive Program” and provided for incentive payments to qualifying physicians of 2 percent for 2009 – 2010, 1 percent for 2011 – 2012 and 0.5 percent for 2013. The percentages were of the allowed charges for all such Physician Fee Schedule (PFS) covered professional services furnished by the eligible professional during the reporting period. Then, starting in 2012, if the eligible professional was not a successful E-Prescriber for the year, incentive penalties of the following amounts would be assessed:
• 1.0 percent for 2012,
• 1.5 percent for 2013, and
• 2.0 percent for 2014 and each subsequent year.
- 2008: Genetic Information Nondiscrimination Act of 2008 (“GINA”). GINA was somewhat of a setback for the use of health rewards. Title I of GINA includes provisions that generally prohibit group health plans and health insurance issuers from discriminating based on genetic information. Thus, under GINA, plans and issuers were generally prohibited from offering rewards in return for the provision of genetic information, including family medical history information collected as part of a Health Risk Assessment (HRA). http://www.dol.gov/ebsa/faqs/faq-GINA.html
- 2010: Patient Protection and Affordable Care Act (“ACA”). ACA section 1201 amended the HIPAA nondiscrimination and wellness provisions of the PHS Act (but not of ERISA section 702 or Code section 9802). As amended by the ACA, the nondiscrimination and wellness provisions of PHS Act section 2705 largely reflect the 2006 regulations (except as discussed later ), and extend the HIPAA nondiscrimination protections to the individual market. [7] These provisions were given real meaning in the passing of the 2013 Wellness Regulations detailed below.
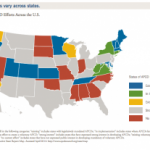
- 2011: Medicaid Incentives for the Prevention of Chronic Diseases (“MIPCD”). Section 4108 of the ACA created the MIPCD program. The grant program provided a total of $85 million over five years to ten states to test the effectiveness of providing incentives directly to Medicaid beneficiaries who participate in prevention programs and change their health risks and outcomes by adopting healthy behaviors. States were required to address at least one of the designated prevention goals: tobacco cessation, controlling or reducing weight, lowering cholesterol, lowering blood pressure, and preventing or controlling diabetes. In September 2011, the Center for Medicare and Medicaid Innovation awarded ten states demonstration grants: California, Connecticut, Hawaii, Minnesota, Montana, Nevada, New Hampshire, New York, Texas, and Wisconsin. States are in the process of implementing their incentive programs and grant funding runs through January 1, 2016. An interim evaluation was conducted in November 2013, and a final evaluation will be completed by July 2016. http://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2011-Fact-sheets-items/2011-09-13.html
- 2011: Medicare and Medicaid Electronic Health Care Record (EHR) Incentive Programs provide incentive payments to eligible professionals, eligible hospitals, and critical access hospitals (CAHs) as they adopt, implement, upgrade or demonstrate meaningful use of certified EHR technology. The programs, which provided for $44,000 under Medicare and $63,750 under Medicaid as outlined below:
|
MEDICARE EHR INCENTIVE PROGRAM |
MEDICAID EHR INCENTIVE PROGRAM |
|
Run by CMS |
Run by State Medicaid Agency |
|
Maximum incentive amount is $44,000 |
Maximum incentive amount is $63,750 |
|
Payments over 5 consecutive years |
Payments over 6 years, does not have to be consecutive |
|
Payment adjustments will begin in 2015 for providers who are eligible but decide not to participate |
No payment adjustments for providers who are only eligible for the Medicaid program |
|
Providers must demonstrate meaningful use every year to receive incentive payments. |
In the first year providers can receive an incentive payment for adopting, implementing, or upgrading EHR technology. Providers must demonstrate meaningful use in the remaining years to receive incentive payments. |
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Basics.html
More Read


- 2013: 2013 Wellness Regulations. On June 3, 2013, the Departments published final regulations to implement PHS Act section 2705 and amend the 2006 regulations regarding nondiscriminatory wellness programs in group health coverage. With respect to rewards, the regulations required that the reward for a health-contingent wellness program, together with the reward for other health-contingent wellness programs with respect to the plan, must not exceed 30 percent of the total cost of employee-only coverage under the plan, or 50 percent to the extent the program is designed to prevent or reduce tobacco use. Like the 2006 regulations, the regulations continued to divide wellness programs into participatory wellness programs and health-contingent wellness programs.
- 2013: Medicare “Better Health Rewards” Act of 2013. Senators Rob Portman (R-Ohio) and Ron Wyden (D-Ore.) introduced the Medicare “Better Health Rewards” Act of 2013, a 100% voluntary program designed to help Medicare beneficiaries get and stay healthy by giving participating seniors achievable goals, a plan to reach them and incentives to keep motivated. This was the first proposal to offer financial rewards for reaching health care goals for Medicare. Medicare Better Health Rewards is a three-year wellness program that uses the annual wellness visit Medicare already pays for to ascertain and measure improvements in six key areas of health: tobacco usage, body mass index, diabetes indicators, blood pressure, cholesterol and up-to-date vaccinations and screenings. In the first year, Medicare beneficiaries who choose to participate in the program will be assessed in each of these areas and then work with their doctor to develop a plan to bring their indicators into a healthier range. The senior’s progress will be measured during subsequent wellness visits in years two and three of the program during which they can earn up to $200 in year 2 and $400 in year 3. Better Health Rewards One Pager.docx (18.5 KBs). The legislation never passed despite support from America’s Health Insurance Plans (AHIP), the Care Continuum Alliance, the Cleveland Clinic, the Cooper Clinic Preventive Medicine, the Healthcare Leadership Council, Deepak A. Kapoor, M.D., Oregon Health & Science University (OHSU), Preventive Medicine Research Institute, Dean Ornish, M.D., Scott & White Healthcare, Dr. Mehmet Oz, Dr. Mark Hyman, The UltraWellness Center, Joel Allison, President and CEO, Baylor Health Care System and Dr. Molly Coye, Chief Innovation Officer, UCLA Health System. http://www.portman.senate.gov/public/index.cfm/wellness-rewards
- 2014: Medicare Regulations.On May 23, 2014, CMS revamped long standing regulations to allow far more flexibility to reward Medicare recipients for healthy behavior including:
- Removing Dollar Limit: removal of the 15 per instance and $50 per year dollar limit per member. CMS did not establish a set maximum dollar limit per activity or per year. Under this proposal, rewards and incentives would be subject to a monetary cap in an amount CMS determines could reasonably be expected to affect enrollee behavior while not exceeding the value of the health-related service or activity itself. CMS did add, though, that if it decides such limits are needed in the future, it will arrange for this through further guidance.
- Expansion of Behaviors: CMS noted that it “would like to enable MA organizations to offer health-driven rewards and incentive programs that may be applied to more health-related services and activities than are allowed under our current guidance.”
- Progress vs. Completion: this authorizes MA plans to grant rewards even if the entire goal has not been reached, instead of the provision limiting such rewards to the “completion of” the program.
- Targeting Conditions: CMS indicated that while the regulations prohibit discrimination, it “would not preclude MA organizations from offering rewards and incentive programs that target a specific disease, chronic condition or preventive service.”
CMS declined to expand this provision to include Part D plans, despite requests from certain commenters that it do so. The revised CMS policies took effect 60 days after the May 23 publication of the final rule in the Federal Register.
The use of health rewards throughout the healthcare community has been a long journey. The progress on the legislative front has been significant, and might be further enhanced by national health rewards legislation that might look like the Healthy America Rewards Act we proposed.
That journey doesn’t end in the United States, as countries throughout the world are following a similar path. See “When It Comes To Health Rewards…It Seems The World Is Flat”
We expect there to be continued use of health rewards including expanded use in the Medicaid arena and hope that the legislative environment will continue to evolve and provide clarity and support for their use in helping to fix the health of America.
health rewards / shutterstock

_9_1-150x150.jpg)
{kind=link}