A publication called “Becker’s Hospital CFO” recently ran a story based on data from a company called DataGen on “The Truth Behind Variation in Episode Payments.” The article claims it will explore “the regional variations in Medicare payments for 90-day episodes of care.” This is to prepare for the new era of bundled payments, which is supposedly right around the corner.
A publication called “Becker’s Hospital CFO” recently ran a story based on data from a company called DataGen on “The Truth Behind Variation in Episode Payments.” The article claims it will explore “the regional variations in Medicare payments for 90-day episodes of care.” This is to prepare for the new era of bundled payments, which is supposedly right around the corner.
 In fact, the article does two things:
In fact, the article does two things:
- It completely fails to explain the regional variations it identifies, and
- It illustrates what a poorly thought-through idea bundling is, especially when designed by payers like Medicare.
The article defines four types of episodes that are likely candidates for bundled payment. These all start with an inpatient admission followed by post-acute care treatment –
- Acute Myocardial Infarction (AMI)
- Congestive Heart Failure (CHF)
- Pneumonia
- Major joint replacement
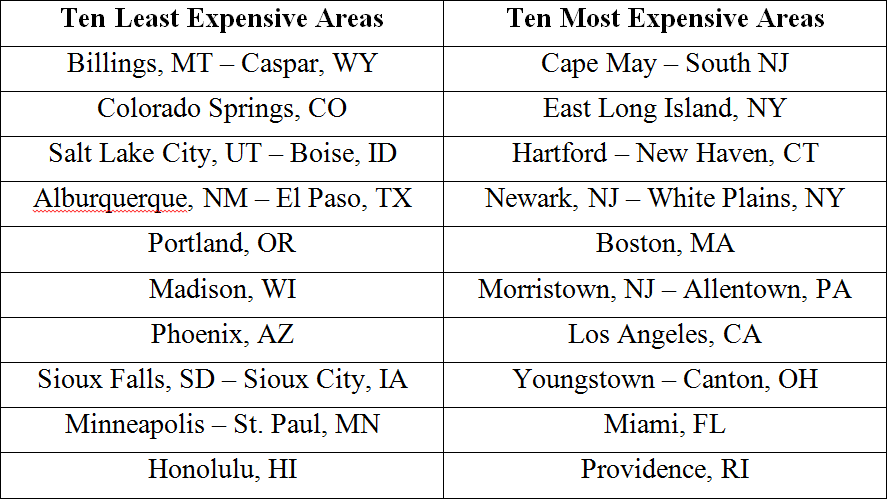
It identifies the ten least expensive and the ten most expensive geographical areas based on Medicare payment. It finds that cost variations are not due to the initial hospital stay, but by the post-acute care treatment. It notes that inpatient service (and payment) is already standardized, but that after-care leaves a lot of room for variation.
For example, in cases of CHF the ten most expensive areas are much more likely to use institutional care following hospitalization and also to have readmissions.
The article goes into much greater detail about the sort of care provided for each condition, and the relative cost of each method. It also charts the geographic areas with the highest and lowest costs.
Not surprisingly, it finds that patients who do “self-care” after inpatient stays are by far the least expensive, those who use a home health agency are the second least expensive. People who are placed a in a SNF, rehab facility, inpatient psych, and so on, are far more expensive.
But it offers absolutely no explanation of why some areas use less expensive settings than others. It seems to assume that some facilities are randomly better able to squeeze expensive care out of the system than others, and that bundled payments will stop that from happening.
Although the report claims it that wants to “provide services to and payment for patient-centered care,” it has no curiosity about whether the needs and resources of patients in Caspar, Wyoming might be different than those in Newark, New Jersey. Perhaps the patients in Caspar are better able to go home and be cared for by friends and family than are those in Newark. Perhaps the providers are simply responding to these varying needs.
We’ve encountered this problem before, especially in the research conducted by the Dartmouth Health Atlas. See hereand here.
Dartmouth couldn’t figure out why terminal patents in Ogden, Utah might be better able to go home to die than those in New York City. It was a complete puzzle to them, so they concluded it must be that hospitals in New York are greedier than those in Utah.
This is the inevitable result when researchers view patients as cookie cutter people. For all the nice rhetoric about being “patient centered,” they couldn’t care less about the actual needs of real people. They want each of us to conform to the population average.






{kind=link}