The latest issue of Health Affairs is devoted to racial and ethnic disparities in the consumption of health care. Naturally, they found some. Why are they there?
The latest issue of Health Affairs is devoted to racial and ethnic disparities in the consumption of health care. Naturally, they found some. Why are they there?
Let’s consider another necessity: food. Suppose you get a Double Quarter Pounder with cheese and a large order of fries, my favorite fast food indulgence when I put all considerations about healthy eating aside. Do you think your burger would have less cheese if you were a black customer? Would your fries be less crispy if you were Hispanic? Would the meat would be less juicy if you earned a poverty level wage?
The answer to these questions is obvious. Just about anybody in America can have the same fast food dinner anyone else in America is having — usually with very little inconvenience. If there is any disparity in this market, it is due solely to individual preference and choice.
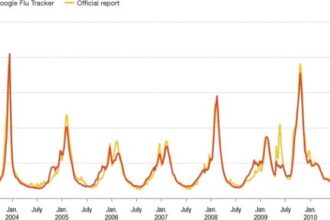
So what makes health care different? I am happy to report that increasingly, it isn’t different. MinuteClinics, RediClinics and other walk-in establishments around the country offer standardized services that are comparable to the market for cheeseburgers and fries. In fact, almost one of every five people who got a flu shot last year got it at a supermarket or a drugstore. At a walk-in clinic, your flu shot costs the same as my flu shot. Your allergy prescription is just as inexpensive and just as accessible as mine. If there is any difference between us it is solely due to differences in needs and preferences. Nothing more.
The Failure of Orthodox Health Policy. So what’s the problem? Almost the entire health policy community is dead set against having medical care delivered in this way. The orthodox view is that (a) markets should be systematically suppressed, (b) medical care should be completely free at the point of consumption and (c) availability should be rationed by waiting and other non-price mechanisms.
Yet wherever the orthodox approach has been followed, disparities are rampant. The Inuit and the Cree in Canada, the Maori in New Zealand, Aborigines in Australia — all have less access to care and worse health outcomes than the majority white populations of those countries. (See the summary in Lives at Risk.)
For the United States, a policy brief on health disparities, produced by the Agency for Healthcare Research and Quality, appears in Health Affairs. Chris Fleming summarizes the report this way:
[B]lacks, American Indians, and Alaska Natives received worse care than whites for about 40 percent of the agency’s list of core measures (which include such criteria as whether women receive timely mammography screenings and whether heart attack patients receive recommended hospital care).
Hispanics or Latinos, meanwhile, received worse care than non-Hispanic whites for about 60 percent of core measures. The agency said the situation was improving, but very slowly. And as for minorities’ access to health care—defined as the ability to obtain care when and where they needed it—about 60 percent of the agency’s core measures did not show any improvement, and 40 percent were getting worse, the agency reported.
Bad as all this appears, the situation here is not worse than it is in other countries. As we have pointed out before, our health care system is probably more egalitarian than most other developed countries, including Canada and Britain.
Disparities Around the World. In the last half century, no country in the world has been more dedicated to the goal of equal access to care than Britain and no country has made a greater empirical effort to monitor its progress in achieving that goal. As we pointed out in Lives at Risk, when the British National Health Service (NHS) was established in 1948:
Aneurin Bevan, father of the NHS, declared that “everyone should be treated alike in the matter of medical care.” The Beveridge Report, the blueprint for the NHS, promised “a health service providing full preventive and curative treatment of every kind for every citizen without exceptions.” The British Medical Journal predicted in 1942 that the NHS would be “a 100 percent service for 100 percent of the population.” The goal of NHS founders was to eliminate inequalities in health care based on age, sex, occupation, geographical location and—most importantly—income and social class.
So how well did it all turn out?
[M]ore than thirty years into the program (in the 1980s), an official task force (the Black Report) found little evidence that access to health care was any more equal than when the NHS was started. Almost twenty years later, a second task force (the Acheson Report) found evidence that access had become less equal in the years between the two studies.
Across a range of indices, NHS performance figures have consistently shown widening gaps between the best-performing and worst-performing hospitals and health authorities, as well as vastly different survival rates for different types of illness, depending on where patients live. The problem of unequal access is so well known in Britain that the press refers to the NHS as a “postcode lottery” in which a person’s chances for timely, high-quality treatment depend on the neighborhood or “postcode” in which he or she lives. “Generally speaking, the poorer you are and the more socially deprived your area, the worse your care and access is likely to be,” says The Guardian, a staunch defender of socialized medicine. Scholarly studies of the issue have come to similar conclusions.
So what is it the British are missing? Three things.
First, the price system is the most equalizing institution ever produced by mankind. A largely unfettered price system is why you and I have roughly the same access, for the same price, to a flu shot at just about any CVS pharmacy. It is why we also have roughly the same access, at the same price, to a Quarter Pounder with cheese at any McDonald’s restaurant.
Second, the British made no attempt to understand the economics of non-price rationing. Third, they made no attempt to understand the economics of discrimination.
The Economics of Non-Price Rationing. As we have previously noted here and here, the major barrier to care in the United States is not price. The most important barriers to care in this country are the same as they are in other developed countries. They are non-price barriers. These include, for example: How long does it take me to make a doctor’s appointment by phone? How long do I have to wait before I can see the doctor? How long does it take to get to and from the doctor’s office? How long do I have to wait once I arrive at the doctor’s office?
Not only are non-price barriers the most important obstacles to care, higher-income, better-educated people find it easier to overcome them than lower-income, less-educated people. In other words, rationing by waiting and other forms of non-price rationing make inequalities worse, not better.
If we want to make health care more accessible — especially to vulnerable populations — we should focus on how to remove, or lessen the impact of, these non-price barriers. Of course the most straightforward way is to substitute rationing by price for rationing by waiting.
This is essentially the way the Food Stamp program works. Instead of making food free (or selling it far below-market prices), we allow the market to determine prices and empower low-income families with Food Stamps (which you can think of as a food vouchers).
The Economics of Discrimination. Thanks to the path-breaking work of University of Chicago economist, Gary Becker, we know a great deal about how institutions affect racial and ethnic discrimination as well as discrimination based on age, sex and other individual attributes.
In a free labor market, employers are able to discriminate at will in their hiring practices. But if the market as a whole is discriminating, each employer who discriminates will be financially penalized for doing so. Suppose that white workers are earning $20 an hour for a certain type of job and equally productive black workers are receiving $15. Then any employer who hires a white worker rather than a black, must pay an extra $5 an hour to satisfy his prejudices. Alternatively, a firm that hires only black workers would have labor costs that are 25% lower than those who hire only white workers.
The market not only punishes those who discriminate, beyond some level discriminating firms cannot survive.
At the time of Becker’s original research on this question, I believe he estimated that white workers were getting a 15% wage premium because of the racial preferences of employers (or the racial prejudices they perceive to be held by co-workers or consumers). I don’t keep up with the literature on labor economics, but I would be surprised if the differential is anywhere near that figure today. For sex discrimination, my understanding is that rigorous studies have never found that the market as a whole discriminates against women. Readers can correct me in the comment section if I’m wrong.
[What about the claim that women earn only 87 cents for every dollar men earn? That difference is explained by differences in hours worked, different occupational choices, etc. There is no industry where women earn 87% of what men earn for doing exactly the same work.]
In a nonmarket environment, things are different. If prices are not free to clear the market, then excess demand or excess supply must be cleared in some other way. In general, if people with a scarce resource are not free to discriminate based on price, they will discriminate by some other means. This is why non-price rationing tends to be especially harmful to minorities.
Without looking at any empirical data, economic theory alone predicts that if minimum wage laws and other labor market restrictions create a labor surplus, the black unemployment rate will be greater than the white unemployment rate. If policies that promote first-dollar coverage create a shortage of medical care, economic theory alone would predict that unmet needs will be greater among black patients than among whites.
If the demand for medical care exceeds the supply, for example, providers can discriminate based on racial, ethnic or sexual preferences and not pay a price for doing so. That may be one reason for the statistics given above. It may also help explain why more than half of all patients waiting for an organ transplant are members of a racial or ethnic minority.
![]()