Editor’s Note: Dan Munro is a contributing editor to Forbes.com. His columns are collected under the heading, “The HealthCare Compass.
Editor’s Note: Dan Munro is a contributing editor to Forbes.com. His columns are collected under the heading, “The HealthCare Compass.
This last week – the widely read Dr. Rob Lamberts lamented the usability of his Electronic Medical Record (EMR) software for his new primary care practice. It’s worth reading (here) as it highlights the larger systemic problem of EMR software generally and then specifically as EMR software is overlaid onto a new payment model.
In Dr. Lamberts case, a software solution – one that was built specifically around billing mechanics (namely ICD-9 and CPT “codes”) – was overlaid onto a new practice model that bills patients a flat monthly fee for “all-they-can-eat” primary health care. Almost all EMR/EHR software has been purpose-built to support billing as the primary function. Clinical data capture is the secondary objective – and the EMR/EHR software vendor landscape is 100% reflective of that priority (as is the entire system). At last count, there were over 600 EHR “vendors” and over 300 that had reported at least one doctor or practice that ”attested” to “meaningful use” with their software (a requirement for HITECH Act payment). To date, we’ve spent over $10B on “digitizing” health records.
More Read

I’m struggling to find the right analogy, but I imagine the effect Dr. Lamberts (and others) are feeling is similar to putting a V-8 engine onto a bicycle. Yes, you could (conceivably) engineer that solution – but why would you – and then why would you expect any kind of usable experience? You simply wouldn’t (unless, perhaps, you were Evel Knievel). Even Felix Baumgarten carefully employed a team of 300 (including 70 engineers and doctors) in his lone (and breathtaking) leap from the edge of space.
Forbes colleague David Shaywitz wrote more broadly (and brilliantly) about this in his piece earlier today: Handle With Care: Success of Digital Health Threatened by Power of Its Technology. This too is well worth worth reading as it relates to the “quick-fix” mentality that is pervasive in both our culture and our wheezing health care system. It’s everywhere – and short-sighted. For providers, let’s cram-down EHR solutions so that we can “capture” the downstream data/analytics that we so desperately need to control costs – with little interest, attention or concern to the consequence on the front-end patient dynamics (including both patient AND provider experience). For employers, let’s add “gamification” and “wellness” programs (with “behavioral economics” of course) to the HR/Benefits equation. While we’re at it – let’s automate low-acuity, primary care as much as we possibly can. There – all done. We’ve digitized, gamified and automated the whole mess.
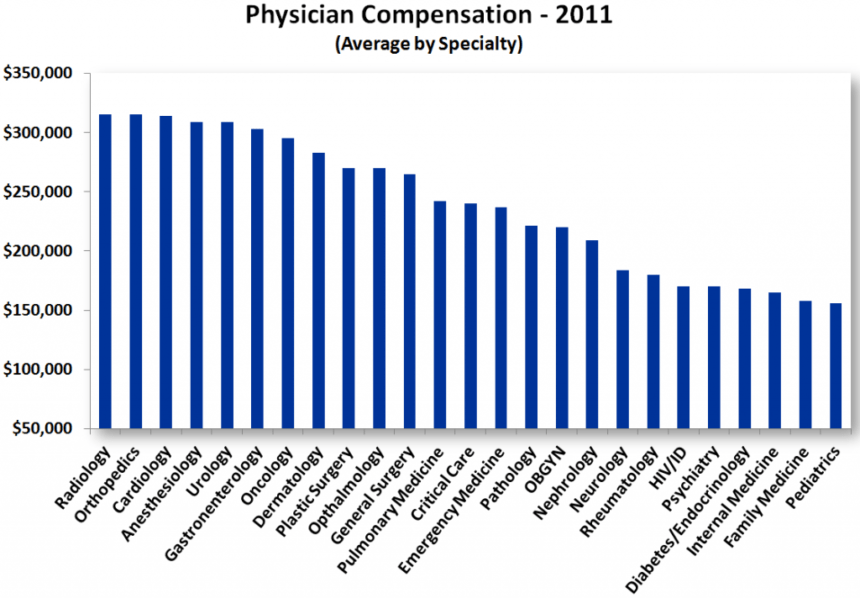
The effect – as evidenced by Dr. Lamberts plight (and flight) – is to eject altogether. The fundamental hope (and risk) of this “direct-to-consumer” model is that personal (and fiscal) sanity will return to the private (often solo) practice of primary care. I’m not sure it’s the right hope (or exit), but I do understand the motivation and it is a worthwhile experiment because, more than ever, we need primary care physicians to stay engaged as we work through our health care transformation. I argue that Medscape’s chart on ”average” physician compensation highlights the broader dilemma – namely that primary care (the very entry point for health care) is the lowest paid.
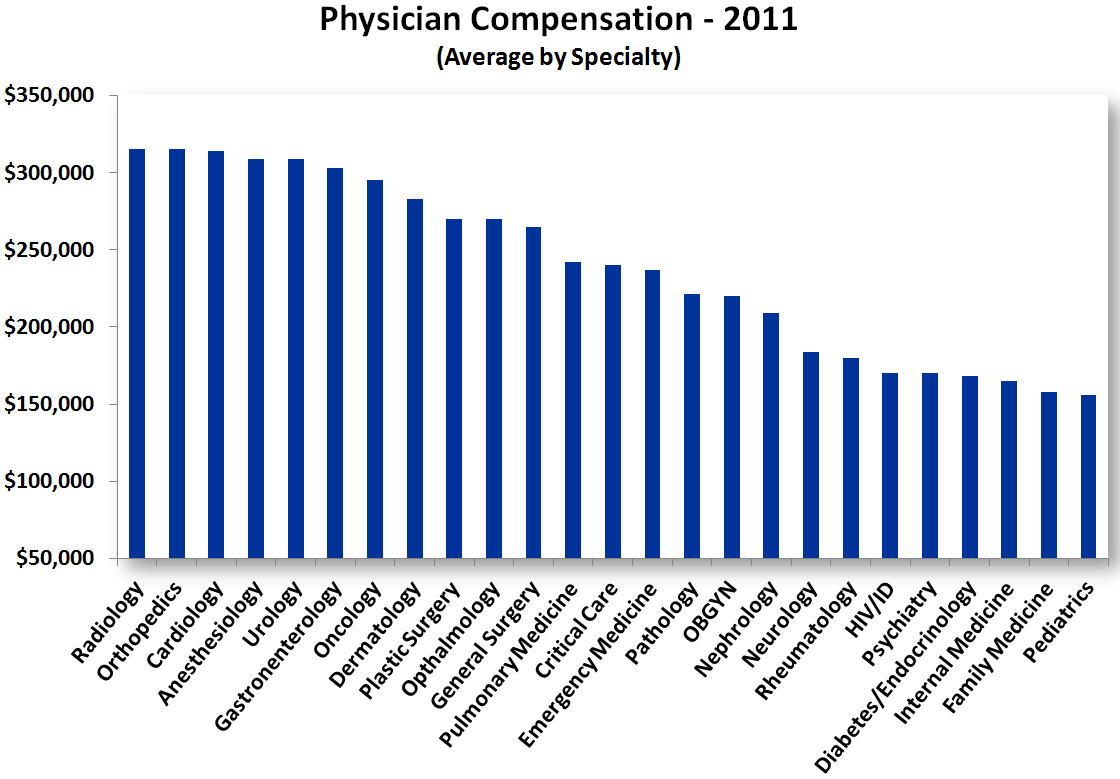
We pay primary care in much the same way that we pay tellers at the bank. Tellers aren’t dead – nor is their survival at risk – but it’s tilting heavily toward the retail economy. So are primary care physicians. These are all the ”gatekeepers.” In fact, that may well be the exact path we’re on as we attempt to automate (and further minimize) the dynamics of primary care. Several companies (eg: Healthspot – which I wrote about in my CES coverage earlier this month) are building the physical Kiosk’s specifically targeting low-acuity, primary care. As a primary care physician – the assault is relentless – from every direction.
- Current payment rates that are unsustainable to a practice
- Further cuts to payment rates in the forecast
- Increasing demand for “accountability” (both regulatory and ACO’s)
- Complete subjugation by other specialties – where primary care is treated as the “funnel” or “filter” to higher-rate specialties
- Kiosk’s and eVisits as the final automation of primary care altogether (do we know who the doc-in-a-box is? Should we care?)
- Ever increasing volume as more people join the ranks of the “insured”
The technology overlay is simply the gamification and behavioral economics to support an increasingly desperate need for lower cost, but it’s unrelated to any metrics that support either better health outcomes or better care delivery. We don’t know. It’s entirely experimental.
All of which speaks to the huge need for more systemic changes around payment reform. As it stands today, the Affordable Care Act (ACA) does little more than tweak the current payment model. Yes, Accountable Care Organizations (a by-product of the ACA) are scaling broadly, but adding a risk component to the payment of care doesn’t fundamentally change the “fee-for-service” model – or mentality. As Paul Levy highlighted, ACO’s are “Neither Accountable nor Caring nor Organized”. Ouch. Yes, provider compensation will absolutely be tied to outcome (including things like “re-admissions”), but is that really the biggest, the best and only lever?
Don Berwick has suggested three ”triple aims.” We all know the first – better care, better health and lower cost, which is the ultimate goal, but there are two others. The second is:
- We can get to better care, better health and lower cost – but we’re going to have to improve our way there.
- The 1st Law of Improvement is that every system is perfectly designed to achieve the results it gets (ie: the current system is performing as built).
- Improvement science is a system science – not an economic science.
The third is that there are 3 types of product improvements (and we need all 3):
- Defect removal (ie: reducing hospital infections, fraud and waste)
- Reducing costs (while leaving the customer the same or better)
- Creating a new product or service (ie: a new model)
Don’s preferred example of a new model is the (Malcolm Baldridge National Quality Award winning) Nuka system in Alaska– but it’s not the only example. I wrote about the success of “worksite healthcare” last year. Using back-of-the envelope math – SAS (#2 for 2013 – and on the list of Top 100 Companies to Work for – 10 times) estimates that they save about $6M per year on healthcare costs. It’s not just lower cost either. They continuously demonstrate much happier, more productive employees – who also enjoy better health.
When describing either model, Nuka or worksite, there is almost no reference to digitized workflow. There is no reference to “gamification” or ”behavioral economics.” There’s also no reference to ”payment risk” or EMR “woes.” There is just improved healthcare – and the result is threefold. Better care, better health and lower cost. Triple aim. It does exist – and there’s even more than one model. We can get there but it’s through improvement. As Don Berwick suggests – that’s a system science – not an economic one. Unless and until we see that – I question how much healthcare transformation we’re actually getting. I’m just asking.






{kind=link}